
Research Article | DOI: https://doi.org/10.31579/2690-8794/063
1 Department of Statistics, University for Development Studies, Navrongo, Ghana.
2 Department of Mathematics and statistics, University of Energy and Natural Resources, Sunyani, Ghana
*Corresponding Author: Abukari Alhassan, Department of Statistics, University for Development Studies, Navrongo, Ghana.
Citation: Alhassan A., Imurana I. and Iddrisu A. Karim (2021) Influence of Determinants of Diabetes on Sexual Quality using Multivariate Analysis of Variance J. Clinical Medical Reviews and Reports. 3(1); DOI: 10.31579/2690-8794/063
Copyright: © 2021, Abukari Alhassan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 19 November 2020 | Accepted: 30 November 2020 | Published: 02 February 2021
Keywords: erectile dysfunction; female sexual dysfunction; MANOVA; international index of erectile function; female sexual function index; diabetes
This paper seeks to give a better understanding of the influence of age, creatinine level, duration of diabetes, glucose level and pulse rate on diabetic-induced sexual dysfunction among people. The study employed two-way MANOVA with balanced samples of 115 each. Prior to the analysis, univariate and multivariate normality, linearity, equality of error and covariance matrices, and multicollinearity assumptions were satisfied. Significance was attained for both sex and marital status (P < 0.05), though their interaction effect was not significant (P > 0.05). Wald’s test for individual groups confirmed the hypothetical decision of MANOVA, though independent T2 failed to report significance for marital status. Under the parameter estimation, it was ascertained that the difference between the groups was in terms of age and creatinine levels of people. The model is also considered credible since bootstrap estimates converged to the empirical estimates. Even though this paper did not exhaust all metabolic and comorbid factors relating to diabetes, it is hoped that it provides an insight into some circumstances in the evolution of diabetes.
Dysfunction of the sexual reproductive system is any sexual abnormality that a person suffers which interrupts normal sexual life [10]. Sexual dysfunction is a feeling of discomfort and often disrupts an individual’s social life [1]. Sexual dysfunction may also be defined as unsuccessful sexual activity with a sexual partner [10].
Since sexual function is an ingredient of healthy lifestyle, any form of dysfunction of the sexual system affect the quality of life of an individual. Sexual dysfunction does not refer to a side effect of ongoing medication or interruption in sexual activity which happens for a short period of time but an occurring problem that affects the individual and has the ability to affect other aspects of his or her life. When one cannot keep a good erection for successful sexual activity it may also be an alarm bell for other health conditions that may need treatment and which, mostly may be alarm bell factor for heart related problems [10].
In a broader perspective, sexual dysfunction has been defined according to the type of disorder and the conditions or circumstances that promote the disorder [10] classified disorders of the sexual function into four main areas, which include; “sexual desire disorders, arousal disorders, orgasm disorders and pain disorders”. These disorders basically influence the reduction in libido or reduction in desire for sexual fantasies.
Sexual dysfunction among men has long been known as a common experience. The experience was initially referred to by National Institute of Health [17], as impotence, with little explanation. Erectile dysfunction is increasingly becoming the object of public concern of late due to the prevalence of the condition and the evolution of remarkable oral therapies such as “sildenafil”, “tadalafil”, “Vardenafil”, among others. In an attempt to define the normal time for a good sexual activity, sex therapists have categorized average time for normal erection before ejaculation, upon certain considerations. According to [18], the average therapists’ response on how long erection should last fell under four definitions; erection that lasts between 3 and 7 minutes is considered ‘adequate’, erection that lasts between 7 and 13 minutes is considered ‘desirable’, erection that lasts between 1 and 3 minutes is considered ‘too short’, and erection that lasts between 10 and 30 minutes is considered ‘too long’.
Erectile dysfunction data is generated based on certain standards such as those set by “International Index for Erectile Function (IIEF)”. The IIEF is an instrument that is commonly used to evaluate the male sexual function [21]. The IIEF questionnaire was developed and validated in 1997, after piloting the final scale of 15 items recommended by a panel of international expects. “The questionnaire was divided into five main domains of the sexual function; six items constituted the erectile, two items each constituted the orgasmic function, sexual desire and the overall sexual satisfaction, and three items constituted the intercourse satisfaction”.
Female Sexual Dysfunction (FSD), unlike the males, is not easy to reconcile due to disparities in perception about sex by women. FSD is a complex combination of disorders, which comprises the body, the mind, as well as other social elements. Hypoactive sexual desire disorder (HSDD), according to [4], is a term which refers to the continuous lack of sexual fantasies, which includes unpreparedness of the mind and body [15] also defined female sexual arousal disorders (FASD) as an increasing inability to attain and maintain successful sexual activity. This may be as a result of inadequate lubrication or lack of sexual excitement. According to them, indicators of sexual arousal consist of muscle movement in the pelvis which translates to insufficient lubrication of the vagina and the dilation of the genitals. Sexual pain disorders (SPDs) are another category of dysfunction in females, defined by Susan (2009), which is characterized by pain during sexual intercourse (dyspareunia). It may be characterized by the recurrent muscle spasm in the pelvic floor muscles that interrupt penis penetration (vaginismus) and pains associated with nonvaginal penetration. FSD is also defined by [25], under international classification of diseases, as “a woman’s inability to experience sexual intercourse as she would wish”.
According to Planned Parenthood (Sex and Sexuality), FSD has to do with the reduction in sexual desire and libido. According to sex therapists, FSD is closely associated with the reduction in female sexual hormones, estrogen, especially in menopausal women. Information about the sexual function of individuals can be obtained through female sexual function index (FSFI). FSD is highly prevalent in recent years with rates ranging from 25% to 65% of women in the “generally defined population” [14]. The diagnosis of FSD has often being done based on the system of “American psychiatric association known as diagnostic and statistical manual of mental disorders” (DMS). This system is best at providing appropriate “classification for psychiatric disorders but lacks the classification power for sexual disorders with organic or mixed etiology” (Basson et al, 2000; DMS-IV 1994). The DMS-IV system captured the FSD under four categories; “hypoactive sexual desire disorder (HSDD), female orgasmic disorder (FOD), dyspareunia (painful sexual intercourse), and female sexual arousal disorder (FSAD)”. Basson (2000) expanded the scope of the DMS-IV due to the broad scope of the “female sexual response cycle”. He therefore defined the female sexual arousal which encompasses subjective mental excitement, increased sensitivity of the genital as well as nongenital areas, lubrication and other sensitive areas of the female sexual system [13] also added that the physical perception of the genital also affects the subjective arousal and therefore advocated for multidimensional approach to measure female sexual function (FSF).
Many of the FSF questionnaires do not meet the current definitions under the psychometric and multidimensionality measurement due to the fact that questionnaires are designed to elicit information about a specific sexual function.
Anorgasmia is an example of orgasm disorders, which describes the persistent delays or absence of orgasm. Menopause may be an associated link to anorgasmia. Exposure of the body to some medications, such as antidepressants has the tendency to delay or even eliminate orgasm. Another sexual disorder, especially with women is sexual pain disorder (dyspareunia). The woman experiences severe pain during sexual intercourse, which is believed to be caused by vaginal dryness in women (lack of sufficient vaginal lubrication), changes in hormonal concentrations due to menopause, pregnancy, or by breast-feeding. This association has been reported by [6].
Priapism in men, is a disorder which is characterized by prolong and painful erection that occurs without sexual activity. It is said to be a condition caused by the inability of the penis to draw blood out of its vessels. The adverse effect of untreated priapism is permanent erectile failure as a result of damaged nerves around the penis. Abusers of medications, especially those relying on aphrodisiacs for sexual fantasies are at a higher risk of Priapism.
In some instances, sexual dysfunction is seen as a risk factor of high blood pressure, hyperglycemia, dyslipidemia, and diabetes, as reported by [24].
As far as this study is concerned, emphasis is on diabetic patients experiencing sexual dysfunction. According to [26], “diabetes or diabetes mellitus refers to a group of diseases that affect how the body uses blood sugar (Glucose). Chronic conditions of diabetes are type 1 and type 2 diabetes. Prediabetes is reversible. Type 1 diabetes is a chronic condition in which the pancreas produces little or no insulin to regulate blood sugar. Type 2 diabetes is a chronic condition that affects the way the body synthesizes glucose. Gestational diabetes occurs in pregnant women, and occurs when the body does not react properly to insulin. Some of the symptoms of diabetes, especially type 1 diabetes, include increased thirst, frequent urination, extreme hunger, unexplained weight loss, fatigue, slow-healing sores, blurred vision, frequent infections, etc. Though type 1 and type 2 diabetes can occur at any age, type 2 diabetes is common in people above 40 years. The risk factors of diabetes include age, family history, weight, race, inactivity, abnormal cholesterol, triglyceride levels and high blood pressure. Drugs such as Glucophage and glumetza may reduce the risk of type 2 diabetes”. This paper considered a cross-section of diabetes patients who were diagnosed at the Tamale teaching hospital in Ghana. Respondents equally responded to questionnaires on assessment of sexual function and sexual quality.
“Creatinine is a waste product from the normal breakdown of muscle tissue, filtered through the kidneys and excreted as urine. The level of creatinine is a test for kidney function. The normal levels of creatinine in blood for men and women are 0.6 to 1.2mg/dL and 0.5 to 1.1mg/dL. Creatinine level of 5mg/dL or more is a sign of severe kidney impairment” [26]. “A normal resting heart rate for adults ranges from 60 to 100 beats per minute (BPM). This implies more efficient heart function and better cardiovascular fitness”. Abnormality sets in if your pulse is consistently above 100BPM [2]. Diabetes can be tested for by either using the method of fasting (drawing blood sample after about twelve hours without food or water), or random (drawing blood sample at any given time). If your “fasting blood glucose test value falls within 100 to 125 mg/dL (5.6 to 6.9) mmol/L, it means you have a type of prediabetes. This increases your risk of developing type 2 diabetes. A level of 126mg/dL (7mmol/L) and higher mostly means that you have type 2 diabetes. Also, if your random blood sugar test value falls around 200mg/dL (11.1mmol/L) or higher, it means you have diabetes. Below 5.6mmol/L is normal blood glucose” [26]. Duration of diabetes is the length of time an individual lives with diabetes after diagnosis.
The data used in this paper was obtained from Tamale teaching hospital. Tamale is the capital city of the northern region of Ghana, West Africa. It is the third largest city with a projected population of 562,919 according to the 2010 population census. It is located about 600km north of Accra and dominated by Muslims. The map of Tamale metropolis showing the district boundaries is displayed in Figure 1.
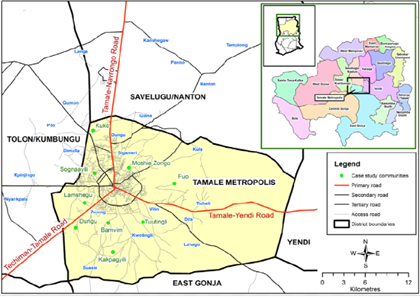
Tamale teaching hospital receives referrals from the surrounding district hospitals such as East Gonja, Central Gonja, West Gonja, Yendi, Savelugu/Nanton and Tolon/Kunbungu districts.
In this section, we discuss the MANOVA and Pearson’s product moment correlation coefficient models used in this paper for investigating the differences between men and women, married and single on some determinants of diabetes. The data was first subjected to credibility tests. Summary statistics were generated afterwards. Finally, the data was subjected to two-way MANOVA.
3.1. Multivariate Analysis of Variance (MANOVA)
Multivariate analysis of variance (MANOVA) is a procedure for comparing multivariate means. It is employed when there are two or more dependent variables. MANOVA is a generalized form of univariate analysis of variance (ANOVA), where sums of squares in the ANOVA are diagonal elements of the covariance matrix of MANOVA. MANOVA helps the researcher to determine the influence of sex and marital status on age, creatinine level, duration of diabetes, glucose and pulse rate.
Some credibility tests under MANOVA include; large sample size, univariate and multivariate normality, linearity, equality of error and covariance matrices, and multicollinearity.
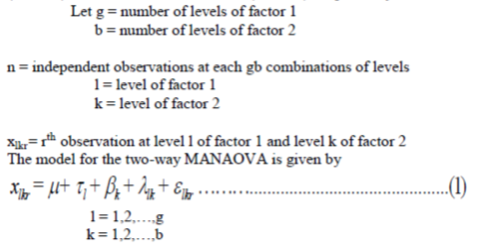
This study deals with two sets of experimental conditions, as level of ‘sex’ (factor 1) and level of ‘marital status’ (factor 2), respectively.







test for the effect of factor 1, factor 2 and factor 1- factor 2 interactions. Wilk’s lambda, is a likelihood ratio test for testing effects of the factors and their interactions, based on the corresponding hypothesis.
Wilk’s lambda,, is given by
3.2. Correlation Coefficient
Pearson product moment correlation (PPMC) is a commonly used parametric statistical tool that is used to investigate the linear relationship between two sets of data. It measures how strong the sets of data are related. The absolute value of the correlation coefficient () is a measure of the strength of the relationship. A correlation coefficient of 1 means that for every increase in one variable, there is a fixed proportional increase in the other. On the other hand, a correlation coefficient of -1 means that for every increase in one variable, there is a fixed proportional decrease in the other. A correlation coefficient of 0 means that there is neither positive nor negative correlation (no relationship) between the sets of data.
The estimate of Pearson product moment correlation coefficient () is given by;

Pearson correlation coefficient is based on the assumption that the dataset is multivariate normally distributed. It is also based on the assumption that the variables are linearly related.
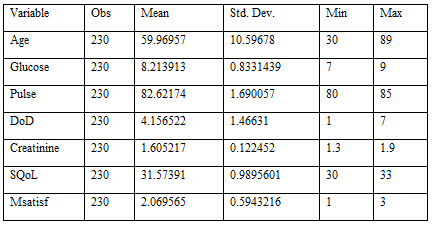
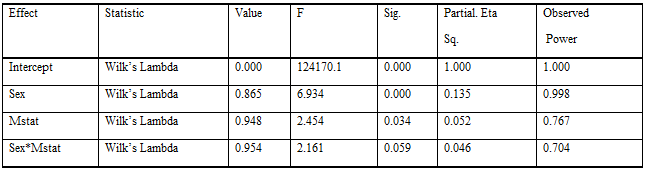
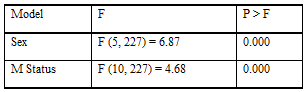
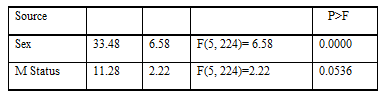
A total of 230 respondents were used in this study. Out of the total number of respondents, 115 (50%) were males and the rest were females. Also, 50% of the respondents were married and the rest were single. Table 1 displays summary statistics for age, glucose, pulse, duration of diabetes (DoD) and creatinine. From Table 1, it can be seen that the average age of respondents is 60 years with the youngest diabetic age of 30 and oldest of 89 years. Similarly, the mean duration of diabetes is 4 years with a minimum of a year and maximum of 7 years. The mean glucose is 8.21ml/dl. The minimum glucose level is 7ml/dl and the maximum is 9ml/dl. The average pulse is 82.62 bpm and the minimum and maximum pulse rates are 80 and 85 bpm, respectively. Also, the average, minimum and maximum creatinine values were 1.6ml/dl, 1.3ml/dl and 1.9ml/dl, respectively. Again, the average scores of sexual quality and marital satisfaction of respondents were 31.6 and 2.1, respectively. From appendix O1, it can be seen that 3.5% of the respondents fall between 30-39years, 12.6% fall between 40-49years, 34.3% fall between 50-59years, 30.9% fall between 60-69years, 18.3% fall between 70-79years, and 0.4% fall between 80-89years. Diabetes can therefore be said to be highly prevalent in adults between 40-79 years old (96.1%). From the two-way MANOVA in Table 3, we noticed that men and women as well as married and single differ significantly. However, their interaction effect is not significant. The powers of the test of the hypotheses are high, indicating high precision. As part of post estimation to confirm the estimates from MANOVA, Wald’s test was used to test the hypothesis of equality of group means. Results from the analysis suggested that the group means are not equal, as shown in Table 4. The post-estimated result is a confirmation to the results of the MANOVA since sex and marital status of respondents were observed to be significantly different. Hotelling test on individual groups revealed that there was significant difference between males and females on the linear combination of Age, Creatinine, Duration of Diabetes, Glucose and Pulse, with a value of 33.48 and P-value of 0.000. On the other hand, there is no significant difference between married and single. This was suggested by value of 11.28 and P-value of 0.0536, as shown in Table 5. Lack of significance for marital status of respondents is a contradiction to MANOVA and Wald’s test of equality of group means.
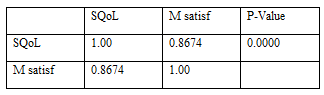
It can be seen that there is high positive correlation between sexual quality of people and satisfaction of their marital union.
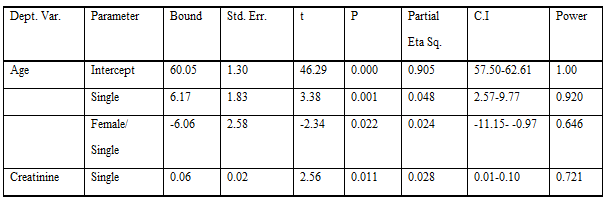
Using the parameter estimation in Table 6, we noticed that the actual difference between sex and marital status is in terms of age and creatinine level of people.
The mean age of the respondents is 60 years, which ranged from 30-89 years. Several studies on sexual dysfunction reported ages ranging between 18-70 years (Molouk et al., 2013; Edward et al., 1999; Katherine et al., 2010). The disparity in the ages might be as a result of the fact that this study encompasses both diabetes and sexual dysfunction. The mean glucose level was 8.21ml/dl, ranging from 7ml/dl-9ml/dl, falling within the diabetic range of between 5.6 - 6.9 [26]. The average pulse rate was 82.6bpm, and ranged from 80-85bpm. Since normal pulse rate is below 100bpm [26], it can be said that diabetes does not independently influence the pulse rate. The mean duration of diabetes was 4.2 years, with a minimum and maximum of 1 and 7 years, respectively. Some studies have reported higher duration of diabetes (Hermans et al., 2009). The mean creatinine level was 1.6ml/dl, which ranged from 1.3-1.9ml/dl. The values reported in this study fell out of the normal creatinine level, affirming diabetes, according to the diabetes literature [26].
Sexual dysfunction among diabetic patients was age related, and that patients between 50-79 years of age mostly experience severe sexual dysfunction. Sexual dysfunction also affects marriage satisfaction. The ability of an individual to sexually satisfy the partner improves their marital satisfaction. While diabetic men and women, single and married differ according to age, only the single differ in creatinine levels. This paper reports that men and women do not differ in the effects of duration of diabetes, glucose levels and pulse rates, on their sexual function. The power of the test for age and creatinine level under sex and marital status is (0.999, 0.779) and (0.678, 0.669), respectively [23]. For age, the mean score for males is lower (58.32) than the females (61.52). Also, for creatinine, the mean score for males is lower (1.586) than in females (1.624). Although, statistically significant, the actual difference in the two mean scores was 3.2 scale points for age and 0.038 for creatinine.
Based on the analysis of the data some credible conclusions have been made. Diabetic men and women, single and married, differ in terms of age and creatinine levels. It may also be concluded that there is a highly positive correlation between sexual dysfunction and satisfactory relationship between couples.
The authors declares that they have no competing interests
II wrote this article with AA, performed the analysis and organized the literature. AA supervised and provided consultation on the analysis and presentation of findings. AI reviewed the paper, provided the data and consulted on ethics approval. The final version of this work was approved by AA.
The author would like to acknowledge Dr. Suleman Nasiru for some vital contributions to this article.
The data used for this study are from the disease diagnostic, treatment and management system, Tamale teaching hospital.
The study received no funding.
Ethics approval (and consen to participate)
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
